


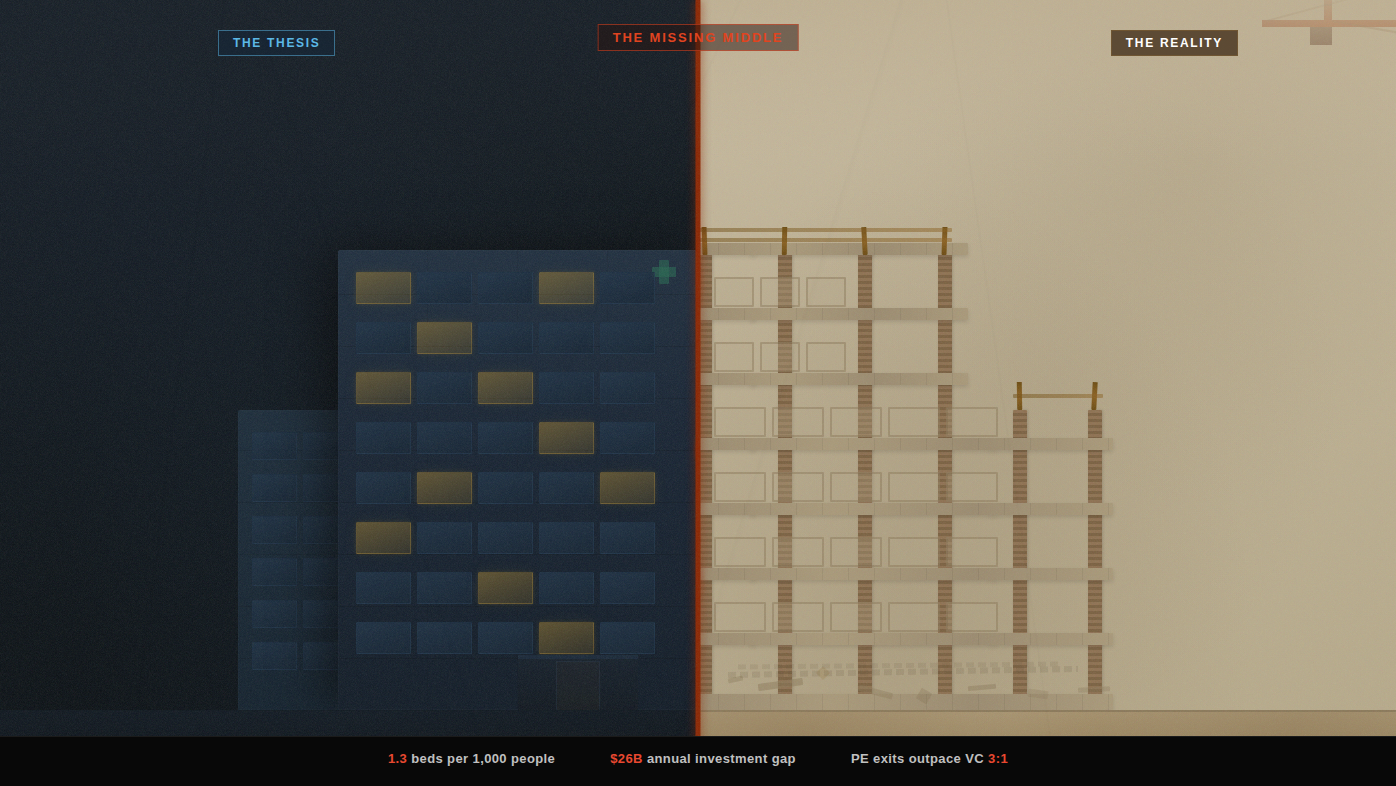
The Skeleton and the Skin
What Nigeria's capital funding collapse means for African healthtech, and why the companies filling the gap are building a private healthcare system from the ground up.
I have been rethinking the "healthtech should follow the fintech model" narrative.
For years, the playbook was simple: look at what M-Pesa did for money, then do the same for health. Build a platform, digitize the process, leapfrog the infrastructure. The thesis sounded elegant. It also assumed a level of existing infrastructure that simply does not exist in most of sub-Saharan Africa.
We are light years away from that model working.
Look at the healthcare businesses on African stock exchanges today or the ones that have attracted serious private equity capital. They are asset heavy. Netcare. Life Healthcare. Fidson. May and Baker. These are not SaaS companies with dashboards and monthly active users. They are companies with factories, hospital beds, cold-chain warehouses, and regulatory licenses tied to physical locations.
My prediction: tech plus assets is the combination most likely to produce a real exit within the African ecosystem. And the data from 2024 and 2025 is starting to prove this out.
But here is the honest version: the thesis is easier to articulate than to fund. And the funding problem is far more brutal than most commentators acknowledge.
Before we talk about who is building what, it is worth pausing on the size of the gap. The African Development Bank's 2022-2030 Health Infrastructure Strategy lays it out starkly: Africa has just 1.3 hospital beds per 1,000 people. Europe has 6.1. Latin America has 2.1. A third of Africans live more than two hours away from any health services at all, and only 51% of primary health facilities in sub-Saharan Africa have access to basic water and sanitation.
The economic cost is staggering. The AfDB estimates Africa loses $2.4 trillion in annual output due to poor health outcomes. African governments currently spend $4.5 billion per year on health capital expenditure. The estimated annual investment needed to meet evolving health needs over the next decade? $26 billion. That is a 5.8x gap.
This is the environment into which "healthtech" has been deployed. It is like trying to run a ride-sharing app in a country without paved roads. The software might be brilliant. But the absence of the physical layer underneath it makes the software irrelevant.
Everybody and their uncle is building software. The barrier to entry is genuinely low. A competent team can build a telemedicine app or an inventory management tool in weeks. Which is exactly why software alone is not a moat.
Distribution and network effects were supposed to be the defensible advantage for digital-first companies. But that distribution thesis was built on an assumption of functioning infrastructure. Roads, electricity, reliable internet, cold-chain logistics, functional regulatory systems. In markets where that infrastructure is patchy or absent, the cost of acquiring and retaining customers for a purely digital product is punishing.
To make the distribution route work in Africa, you would need to own the majority of market share across the continent. That is a tall order when your product depends on a physical layer you do not control.
Consider the pharmaceutical market alone. McKinsey projected that Nigeria's pharma market could grow at 9% annually to reach $3.6 billion by 2026, making it comparable in size to South Africa's market. Pharma West Africa now estimates it at $4.5 billion and growing at 9% annually. But 70% of drugs consumed in sub-Saharan Africa are imported, and Africa has fewer than 400 drug manufacturers serving over 1 billion people. China and India, countries with comparable populations, have 5,000 and 10,500 manufacturers respectively. The infrastructure is not just thin. It is almost entirely absent in critical nodes of the value chain.
According to AVCA's 2024 African Private Capital Activity Report, Africa recorded 63 private equity exits in 2024, a 47% increase from the prior year. Meanwhile, venture capital equity funding declined roughly 25% year-over-year and has fallen over 50% from the 2022 peak. Deal volume dropped 22%. Only 26 venture-backed exits materialized in 2024, and trade sales accounted for 84% of all exits since 2019.
Africa's exit-to-investment ratio sits at 0.13x. That means for every dollar deployed into venture, roughly 13 cents came back. Mature markets typically recycle 60 to 80 cents on the dollar within the same timeframe. The liquidity gap is not theoretical; it is structural.
PE firms are the ones actually writing exit checks. And PE firms want tangibles.
The headline transactions of 2024 and 2025 in African healthcare tell a consistent story: buyers are paying for physical footprint, not code.
The pattern is unmistakable. The money is flowing toward physical infrastructure with a technology layer, not technology platforms hoping to plug into a physical layer that does not exist.
It is tempting to point to certain large-ticket healthcare infrastructure deals as evidence that the capital markets are finally aligning with the "tech plus assets" thesis. But intellectual honesty demands a closer look.
On paper, this looks like a textbook blended finance deal. In practice, it is something quite different.
NSIA is essentially public money. The government almost certainly provided guarantees that make this possible, which is why the financing terms are favorable in ways no private healthcare company could replicate. More revealing is the IFC's own project disclosure: the investment will be complemented by IFC advisory services to "assist MedServe expand health access to the poor and vulnerable" and to assess and strengthen "the impact of MedServe's oncology service on a sustainable basis." When the IFC itself is providing advisory support to help the investee become sustainable, this is not a commercial investment. It is a development intervention with commercial trappings.
This matters for the thesis because the MedServe deal cannot be a model for private companies. The government cannot subsidize every healthcare infrastructure play through sovereign guarantees. It can fund one. Maybe two. But the market needs hundreds.
Fintech is supposed to be the success story. And in many ways it is. But the "fintech model" as a template for healthtech falls apart on closer examination.
Fintech "leapfrogged" traditional banking infrastructure because money is fundamentally digital. You can move value as information. Health is stubbornly physical. You cannot download a blood transfusion. You cannot cloud-compute a surgical procedure. You cannot stream an MRI.
Even the fintech exits we celebrate are thin on the ground. Since 2019, Africa has produced just 138 venture-backed exits total across all sectors. If fintech, the "easiest" vertical to digitize, is still struggling to produce consistent large-scale liquidity events, then healthtech will not get there by ignoring the physical reality of the continent.
And notice what the "successful" fintechs have done to stay relevant: they moved into agent networks. Physical infrastructure. Wave, Flutterwave, M-Pesa. The digital product got them started, but the physical distribution network is what made them sticky.
There is a company outside healthcare that perfectly illustrates the operational logic of the "tech plus assets" model: Chowdeck.
While Jumia Food and Bolt Food exited the Nigerian market in 2023 and 2024, Chowdeck thrived. By August 2025, it had raised a $9 million Series A, reached 1.5 million customers, onboarded over 20,000 riders, and started building 40 dark stores across Nigeria.
The dark store pivot is the crucial detail. Chowdeck started as a pure logistics play, connecting restaurants to riders to customers. Asset light. But CEO Femi Aluko (formerly a Principal Engineer at Paystack) recognized a ceiling: "We ventured into delivering groceries and delivering medicines, and we saw that it was increasingly difficult to achieve under 30-minute delivery with supermarkets and pharmacies."
The solution was not a better algorithm. It was physical warehouse space. Owned inventory. Controlled fulfillment.
If the "tech plus assets" model is so compelling, why have companies pursuing it also struggled or failed? The answer is not the model. It is the funding structure.
54gene is the cautionary tale. The value proposition (African genomics) was world-class. The science was real. At its peak, the company had built Africa's largest independent biobank, collecting genetic material across 300 ethnic groups, amassing over 200,000 unique human samples. It generated more than $20 million in revenue from its COVID-19 testing infrastructure alone. But the capital structure was fatally mismatched.
Early-stage money came from Silicon Valley VCs at SaaS-like multiples. That $45 million was then spent on sequencers (a single piece of biotech equipment can cost up to $1 million), lab equipment, cloud storage, reagents. All dollar-denominated. Revenue came in naira. By mid-2022, the company had burned through its capital, slashed salaries, and instituted layoffs. Three CEO changes in one year followed. By July 2023, it was winding down entirely. A Federal High Court in Lagos is now adjudicating who owns the biobank and the genetic data of 100,000 Nigerians.
And here is the uncomfortable truth: the very companies that exemplify the "tech plus assets" model often only got to build those assets because of the unrealistic VC expectations that this thesis critiques.
The textbook answer to the valuation bridge is blended capital: equity for the technology layer, debt for the infrastructure. Separate the capital stack so the tech valuation stays clean for growth investors while the physical assets are financed by capital sources that understand long payback periods.
In theory, this is elegant. In practice, the blending is random, unpredictable, and brutally difficult.
Start with the debt side. Nigeria has infrastructure debt funds. The FSDH Infrastructure Debt Fund was established as a ₦200 billion shelf programme registered with the Securities and Exchange Commission, explicitly targeting healthcare alongside transportation, energy, and ICT. Chapel Hill Denham's Nigeria Infrastructure Debt Fund (NIDF), also a ₦200 billion programme and the first listed infrastructure investment trust in Nigeria and sub-Saharan Africa, has been operating since 2017 with zero non-performing loans across 24 infrastructure investments, including healthcare projects. Its units are listed on the Nigerian Exchange, and it has returned 155% since inception.
These instruments exist. But their existence does not mean they are accessible to the companies that need them most. These funds target established, cash-flowing projects with predictable returns. They are not writing checks to Series A healthtech companies that need to build their first diagnostic center.
So where does that leave us? With a funding gap that has a specific shape:
I want to be careful not to present the "tech plus assets" thesis as a clean investment narrative when it is really a messy operational reality.
The thesis is correct: infrastructure is the moat, and technology is the multiplier. The exits prove it. Goodlife Pharmacy sold for a premium because it had 150 storefronts, not because it had an app. Grinta acquired Citi Clinic to own care delivery, not to improve its marketplace algorithm. MYDAWA raised $9.6 million specifically to open physical stores.
But the path to building that infrastructure is not a slide deck with clean capital allocation buckets. It is a founder spending years doing manual work, generating just enough revenue to prove the model, cobbling together funding from sources that were never designed to work together, and hoping the debt markets mature fast enough to catch up with the opportunity.
For founders, this means the "tech plus assets" model demands a specific temperament. You need the patience to build slowly with whatever capital you can access, the discipline to keep the technology layer lean while you assemble the physical footprint, and the stomach for years of grinding before the capital markets recognize what you have built.
For investors, the implication is that the returns in this space will not come from pattern-matching to Silicon Valley playbooks. They will come from understanding the specific, often idiosyncratic, capital needs of infrastructure-building companies and from being willing to structure deals that do not fit neatly into any existing fund mandate.
For the ecosystem, the biggest need is not another VC fund or another DFI programme. It is the connective tissue between them: instruments that can fund the build-out phase for companies that have proven their model but are not yet at the scale that infrastructure debt funds require. Whoever solves this, whether through venture debt, revenue-based financing, or some structure that does not yet have a name, will unlock the real wave of "tech plus assets" companies on the continent.
I do not think this is the only viable model for African healthtech. Software-only companies can succeed in narrow niches where the physical infrastructure already exists or where the product is truly information-native.
But for anything that touches the actual delivery of healthcare, manufacturing of medicines, diagnostic testing, or supply chain management, the evidence points in one direction. The winners will be companies that build or control physical infrastructure and use technology to make that infrastructure more efficient, more compliant, and more scalable. And the real bottleneck is not the lack of good companies or good technology. It is the absence of a systematic funding pathway from idea to infrastructure at scale.
Investors are experiencing what I would call "paper unicorn fatigue." They have watched hundreds of dashboards get built while maternal mortality rates and drug availability numbers barely moved. The next generation of investment will flow toward companies that can demonstrate both technological capability and physical presence.
The question is whether the capital markets will evolve fast enough to fund them.
Next in this series: I will break down how one company is applying the "tech plus assets" model in practice across the pharmaceutical quality and compliance value chain, from regulatory platforms to modular laboratories and bioequivalence centers. What does it look like to actually build this way, and how do you fund it when the capital markets are not designed for it?
Research-driven writing on healthcare, technology, policy, and the systems that shape care across Africa.










Member discussion